Help your patients see the big picture
Download an action planIs suppressing the ovulatory cycle enough?
In an international, multicenter survey of patients treated in tertiary care centers (n=931), it was reported that

endometriosis patients experience unresolved pain despite management1
According to American College of Obstetricians and Gynecologists (ACOG) guidelines:
Persistent symptoms after first-line failure in patients with suspected endometriosis are one reason to move from initial treatment options and consider a confirmatory laparoscopy or other suppressive therapy.2
Stopping the menses to reduce dysmenorrhea may not be enough to comprehensively address endometriosis pain.
Endometriosis should be viewed as a chronic disease that requires a lifelong management plan according to the American Society for Reproductive Medicine (ASRM)3
Endometriosis treatment goals3:
- Maximize the use of medical treatment
- Avoid repeated surgical procedures
Endometriosis treatment approach2,3
Below is information from ACOG and ASRM to begin your patient assessment*
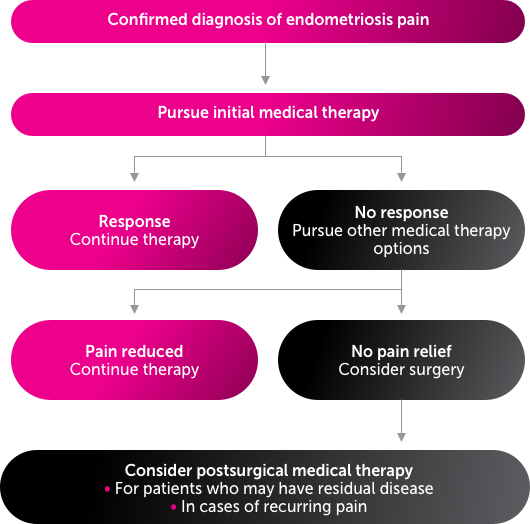
*Adapted from ACOG and ASRM. This is not intended to direct your management plan.
Therapeutic options for management of endometriosis pain2-11
References:
1. De Graaff AA, D’Hooghe TM, Dunselman GA, Dirksen CD, Hummelshoj L, WERF EndoCost Consortium, Simoens S. The significant effect of endometriosis on physical, mental and social wellbeing: results from an international cross-sectional survey. Hum Reprod. 2013;28(10):2677-2685. 2. American College of Obstetricians and Gynecologists. Practice bulletin no. 114: management of endometriosis. Obstet Gynecol. 2010;116(1):223-236. 3. Practice Committee of the American Society for Reproductive Medicine. Treatment of pelvic pain associated with endometriosis: a committee opinion. Fertil Steril. 2014;101(4):927-935. 4. Kodaman PH. Current strategies for endometriosis management. Obstet Gynecol Clin North Am. 2015;42(1):87-101. 5. Ezzati M, Carr BR. Elagolix, a novel, orally bioavailable GnRH antagonist under investigation for the treatment of endometriosis-related pain. Womens Health (Lond). 2015;11(1):19-28. 6. Ng J, Chwalisz K, Carter DC, Klein CE. Dose-dependent suppression of gonadotropins and ovarian hormones by elagolix in healthy premenopausal women. J Clin Endocrinol Metab. 2017;102(5):1683-1691. 7. Struthers RS, Nicholls AJ, Grundy J, et al. Suppression of gonadotropins and estradiol in premenopausal women by oral administration of the nonpeptide gonadotropin-releasing hormone antagonist elagolix. J Clin Endocrinol Metab. 2009;94(2):545-551. 8. Knudtson J, McLaughlin JE. Female reproductive endocrinology. Merck Manuals website. https://www.merckmanuals.com/professional/gynecology-and-obstetrics/female-reproductive-endocrinology/female-reproductive-endocrinology. Updated March 2019. Accessed June 10, 2019. 9. Danocrine [package insert]. Bridgewater, NJ: Sanofi-Aventis. US LLC; 2011. 10. Lupron Depot [package insert]. North Chicago, IL: AbbVie Inc; 2018. 11. Giudice LC. Clinical practice: endometriosis. N Engl J Med. 2010;362(25):2389-2398.